In Part 1 of this two-part series, we learned that Pfizer obfuscated a serious reaction in the clinical trials used to approve the Prizer COVID-19 vaccine for ages 12 to 15.
In Part 2 of this series, we will learn how the FDA ignored its own information protocols and allowed vaccine manufacturers and the press to artificially inflate the perceived benefit of the vaccine for the general population.
Is the Pfizer injection effective in comparison to the risks?
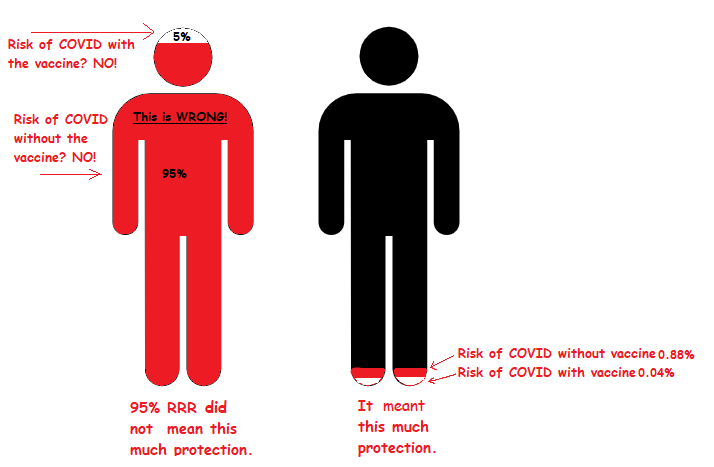
The world celebrated when Pfizer reported 95% efficacy for their vaccine. But the media didn’t clarify that this was the Relative Risk Reduction (RRR) and not the Absolute Risk Reduction (ARR), which was a mere 0.84%. What does this mean?
In the Pfizer trial, 8 out of 18,198 vaccine recipients contracted COVID. In the placebo group, 162 out of 18,325 people contracted COVID. So, according to the data they provided, there was a reduction in COVID cases. However, the overall risk of contracting COVID-19 was already small in the study population -- 0.88% vs. 0.04%.
This distinction is important because the overall benefits of treatment must be weighed against the overall risks.
Do the benefits of the COVID-19 vaccine outweigh the risks in the real world?
It’s disputed that the vaccine reduced infections per 100,000 from 880 to 40. This isn’t just because severe adverse reactions were misclassified during the study but also because PCR tests have been recalled for lack of accuracy.
However, even if we assume the study statistics provided were accurate, the data would mean that they were willing to subject the entire world to a barely tested drug with no longitudinal safety data to reduce the actual risk of catching COVID by 0.84%. These aren’t deaths prevented, but simply the cases of COVID prevented from the slightest sniffle to the rare cases of hospitalization and death.
The risk of death from COVID was already small. The observed case fatality ratio is 1.2%, but this number is inflated like the relative risk reduction vs. the absolute risk reduction. It only applies to the people who actually caught COVID. The overall fatality rate from COVID in the U.S. is only 0.28%. So if there are numerous adverse reactions from the vaccine, do the benefits outweigh the risks?
Consider that 0.3% of COVID vaccine recipients have allergic reactions or anaphylaxis after the first shot. This means that roughly 300 people out of 100,000 will have an allergic or anaphylactic reaction to the first shot.
So, according to the study data offered by Pfizer in its 95% efficacy reports, 300 people would suffer allergy or anaphylaxis for 840 to be protected from catching COVID. Another 0.2% will suffer allergic reaction or anaphylaxis from the second shot. This is 500 cases of allergy or anaphylaxis total to prevent 840 people from simply catching COVID, 1.2% of which might die according to case-fatality data, or 10.8 people.
And the injection is only said to be effective for a few months.
Consider that this is just one simple adverse reaction. We have witnessed massive adverse events from this injection, including debilitating neurological issues, myocarditis and death.
This is why Absolute Risk Reduction is necessary to weigh the benefits of a drug against the risk in the general population.
The FDA recommends using both RRR and ARR to explain risks too.
In short, the press greatly exaggerated the benefits of the COVID vaccines while massively minimizing the side effects in comparison. Please see this short video for a more thorough explanation of RRR vs. ARR and how these measurements affect informed consent.
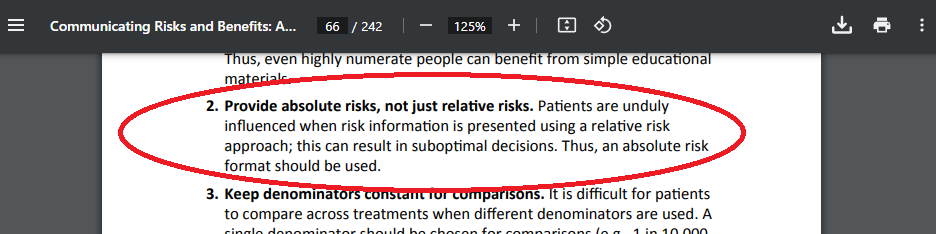
Because it’s easy for laymen to be misled by such unethical tactics, the FDA strongly advises that researchers ``[p]rovide absolute risks, not just relative risks. Patients are unduly influenced when risk information is presented using a relative risk approach; this can result in suboptimal decisions. Thus, an absolute risk format should be used.” (see page 60)
Reuters produced a fact check arguing that RRR should be used to judge efficacy in glaring opposition to this FDA recommendation. The article ignores the above-explained overall risk vs. benefit. It should also be noted that James C. Smith, chairman and former CEO of the Thomson Reuters Foundation, is a board member of Pfizer.
At least 1 out of 1,131 children had a very severe reaction.
Only 1,131 children aged 12 to 15 received the vaccine in Pfizer’s clinical trial. At least one of those participants, Maddie, suffered severe, debilitating effects from the injection.
Per Maddie’s experience, there’s at least a 1 in 1,131 risk of debilitating side-effects from the injection for 12 to 15-year-olds. This translates to 88 per 100,000. For perspective, the current death rate from COVID in the U.S. ranges from 1.32 deaths per 100,000 population in Ohio to 0.23 deaths per 100,000 in Montana. And as explained above, the overall fatality rate in the U.S. general population is 0.28%. The risk for children is even smaller and is zero in children with no comorbid conditions like leukemia.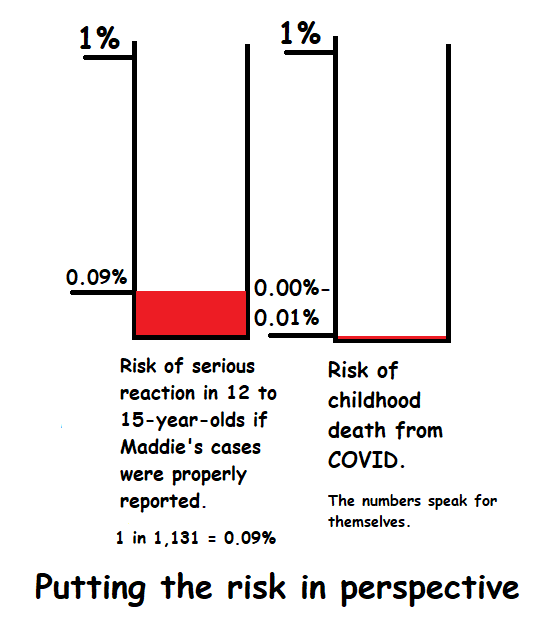
This current scenario perfectly demonstrates why it’s unethical to use only Relative Risk Reduction analysis when promoting pharmaceutical products to the general public, even if the former COO of Thompson Reuters and now board member of Pfizer influences the press to argue otherwise in defense of its product.
It’s also a very effective demonstration of why the institutional imperative is a danger to us all.
Where there is risk, there must be choice.
The COVID-19 vaccine is, by definition, a mass medical experiment because there is no long-term safety data. There can’t be any long-term safety data until sufficient time has passed. The people who participated should have been fully informed of the risk, and the fact that they were not is a crime against humanity.
The result is that countless humans are suffering the effects of a medical treatment campaign that failed to weigh the risk of treatment in proportion to the risk of the disease.
The COVID-19 vaccines were mandated for the general population based on flawed data and flawed reasoning in glaring violation of the FDA’s own stated policies for communication of risk and informed consent.
The press “fact-checks” vaccine information even though they have blatant conflicting interests.
The CDC continues recommending boosters even as COVID mutates far beyond the alleged reach of this injection.
Patients are denied life-saving transplants and other medical care because they refuse to take the injection.
Men and women throughout the Western world are losing jobs, rights and are even being killed for protesting the vaccine mandates.
At the same time, the manufacturers pocket unprecedented liability-free profits while the injuries continue to stack up.
But the situation is far from hopeless.
Our Founders knew that we would face tyranny again one day. It was not a matter of if, but when. They gave us a peaceful option to right these wrongs.
A Convention of States can end the cronyism that destroys our quality of life. We can rein in these regulatory agencies and wrest our nation back from the grip of Big Pharma.
Seventeen states have already joined the call for a Convention of States, and more are joining right now. Get involved by signing the petition at Convention of States.
